What are Annular Fibrin Injections?
A targeted, minimally invasive treatment that uses the body's own biological processes — no surgery, no hardware, no hospitalization.
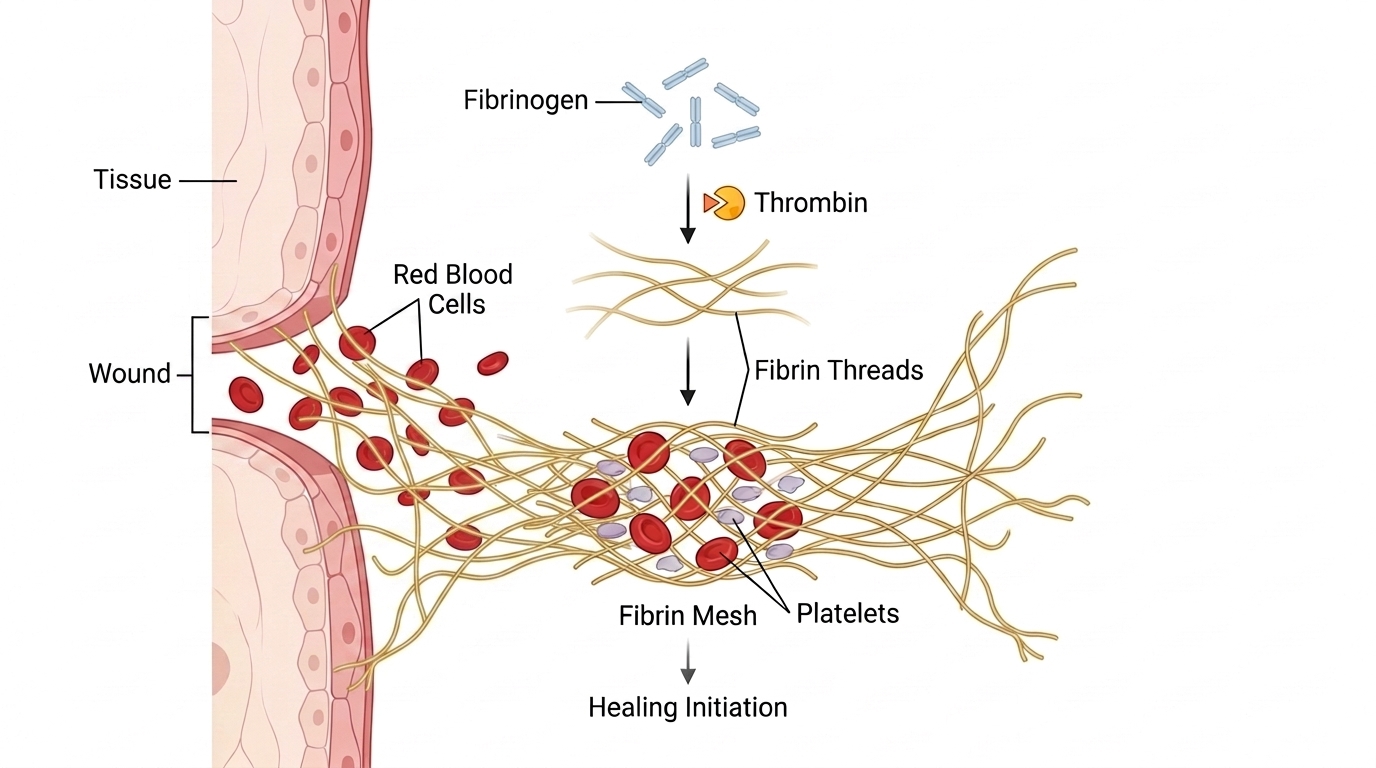
Fibrin is the body's natural structural protein used in wound healing. First identified in 1666 by Italian scientist Marcello Malpighi, fibrin forms when the body activates fibrinogen — a protein that lies dormant in the blood until injury triggers it to assemble into a tough, insoluble fiber mesh. When you bleed, that mesh becomes the framework of a blood clot — sealing the wound and initiating repair. Fibrin has been used in medicine since World War II — first applied to soldiers with battlefield wounds. The modern commercial form has been FDA-approved since 1998, indicated to control bleeding and seal tissue when conventional techniques fall short. AFI applies the same protein, fibrin, to the damaged spinal disc.
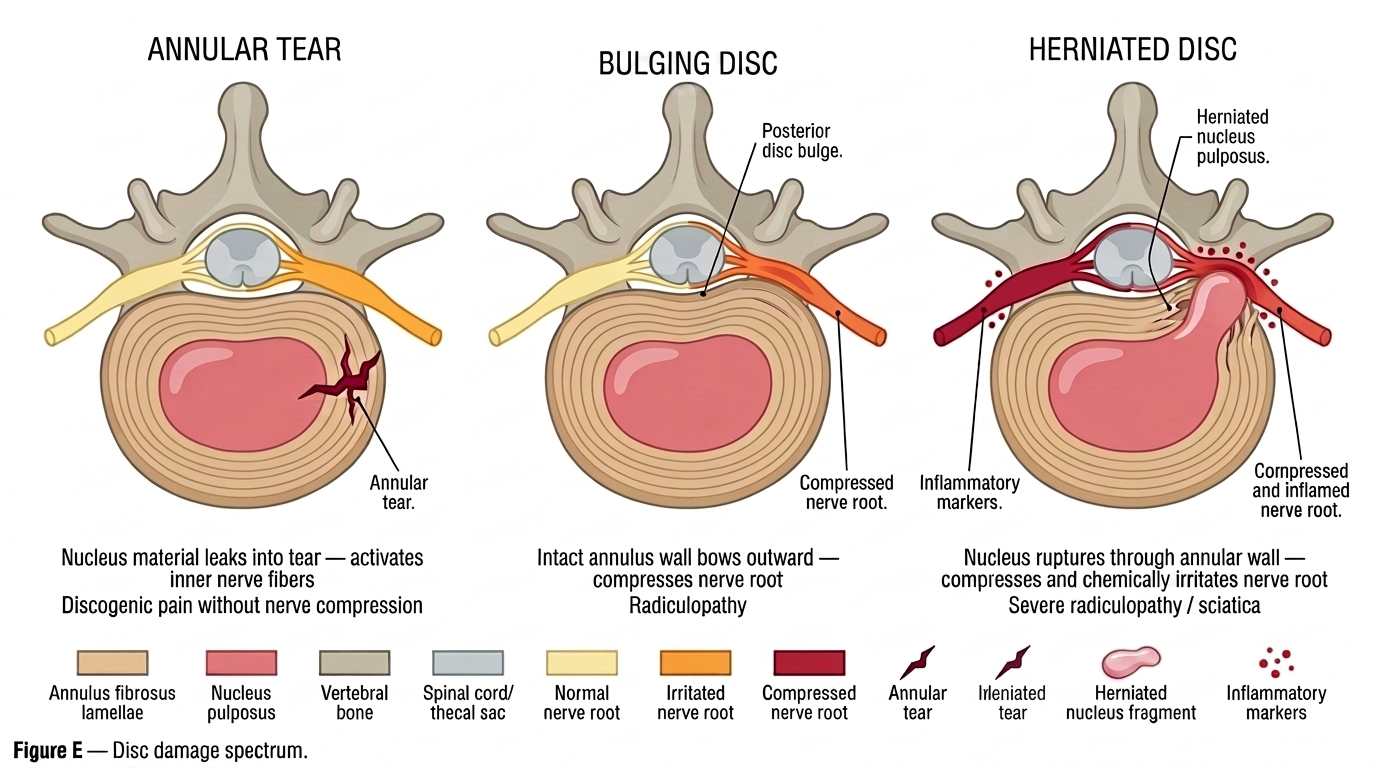
The spinal disc has two components: an outer ring — the annulus fibrosus — and an inner core — the nucleus pulposus. The annulus fibrosus is built from layered collagen fibers arranged in a cross-hatch pattern, giving the disc its strength and the ability to withstand the forces of movement and load. The nucleus pulposus, by contrast, is a gel-like core of water, proteoglycans, and collagen that acts as a shock absorber, distributing compressive forces evenly across the disc. When the outer ring tears or weakens from injury, the disc can bulge outward, herniate, or allow the inner material to leak and irritate nearby nerves. Any of these can cause significant chronic back pain and radiculopathy. Unlike bone and muscle, the disc is avascular, lacking a direct blood supply, and may not easily heal. If these injuries do not respond to non-operative care, one can consider annular fibrin injections.
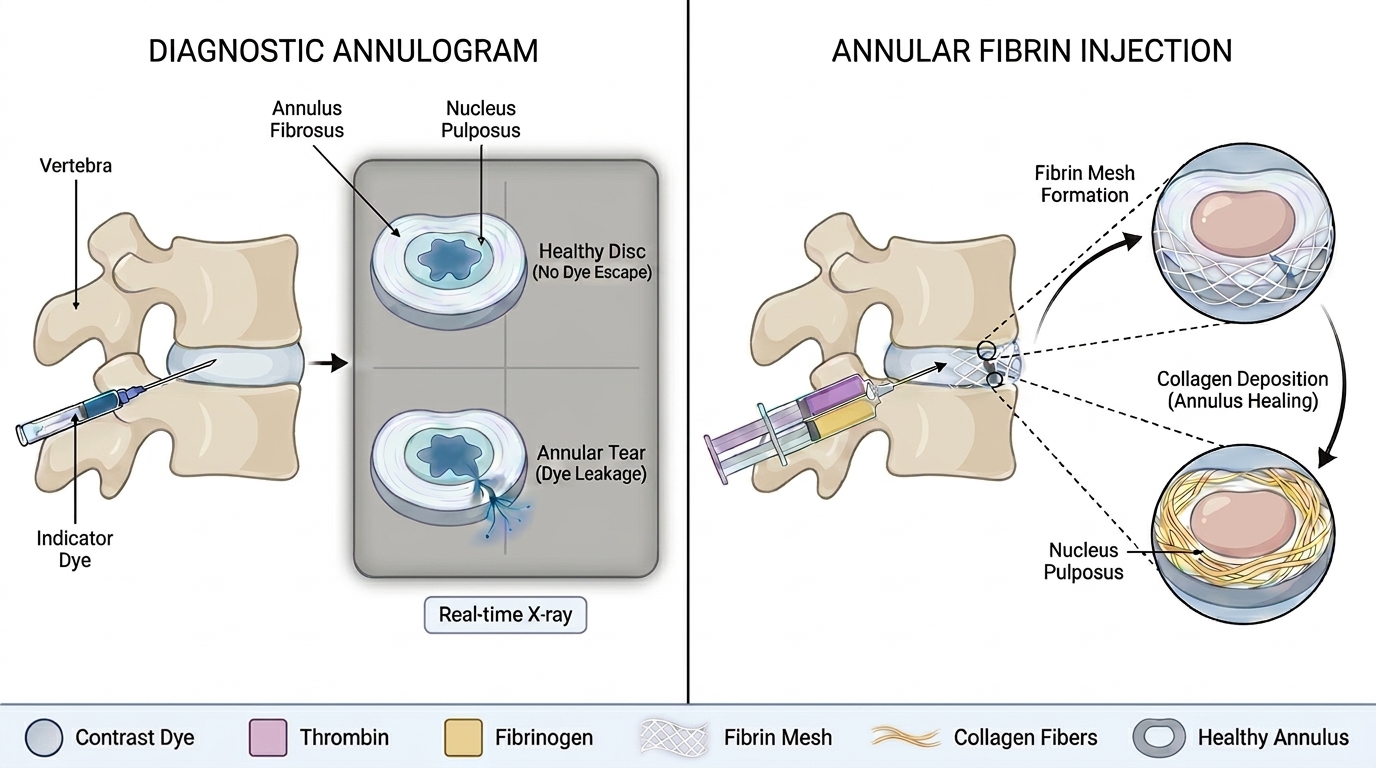
Diagnostic Annulogram: A contrast dye is injected into the annulus fibrosus under live X-ray guidance. Dye that escapes through the annulus confirms the location and extent of the tear — identifying pathology that MRI alone may not identify.
Fibrin Sealant Injection: Through the same needle access, fibrin sealant is delivered into the damaged annulus. The components polymerize instantly on contact, forming a viscoelastic fibrin mesh that seals the annular defect and creates a biological scaffold — stimulating collagen deposition and natural tissue repair.
Pauza et al. (2024), an 827-patient prospective registry, showed sustained, statistically significant improvements in pain and function through 36 months. At 12 months, 50% of patients achieved a Minimal Clinically Important Difference in the Oswestry Disability Index — of those, 74% saw ≥50% improvement and 40% saw ≥75% improvement. Patient satisfaction was 67–74% across all follow-up points, and function scores improved by more than 30% at 6 months, sustained through 3 years.